Proudly Canadian

Richard Reznick
|
In October 2009, at the annual
congress of the American
College of Surgeons, Robin
McLeod, a Regent of the ACS,
organized a symposium on the
Canadian Health Care system.
The room was packed, predominantly
with American surgeons.
By coincidence, as we
were speaking, the U.S. Senate
was voting on Obama's health care reform bill.
The speakers, Rich Finley from the University of
British Columbia, Bill Fitzgerald President of the Royal
College, Hugh Scully from University of Toronto and I
were poised for a backlash of anti-Canadian health care
sentiment. After all, these past few months have seen a
lot of scare-mongering propaganda, such as rumours of
Canadian Death panels (1) and claims that Canadian doctors
are deserting the profession en masse (2).
To our amazement, the reception we received was exactly
the opposite. Our surgical colleagues were profoundly
interested in our comments, by and large not very
knowledgeable of our system, and somewhat in awe of
the messages they received. Without question, most in
the room left with what we believe is the right information;
that Canadian surgeons are for the most part very
pleased with our system and academic health care in
Canada is thriving.
THE MESSAGES
The four speakers described the Canadian health care
system with a focus on the academic health science centre.
We emphasized that the Canada Health Act ensured
Canadians of a system that is universal, portable, accessible,
comprehensive and publicly administered. Rich
Finley commented on the fact that when polled on
who they most respected, more Canadians mentioned
Tommy Douglas, the father of Medicare, than any
other figure. Roy Romanow, in his 2002 report articulates
what many Canadians feel about our system: "the
principles of the Canada Health Act began as simple
conditions attached to federal funding for medicare.
Over time, they became much more than that. Today,
they represent both the values underlying the health
care system and the conditions that governments attach
to funding a national system of public health care. The
principles have stood the test of time and continue to
reflect the values of Canadians."
Our audience was especially interested in the differences
between the Canadian and the U.S. systems. We
acknowledged that those Americans who are insured
enjoy better and more immediate access to health care
services. Further, we underscored that repeated public
opinion polls increasingly have shown that the greatest
concern Canadians have about the existing publicly
funded health care system is the perceived waiting times
for diagnostic services, hospital care, and access to specialists.
But better access to services in the U.S. comes
at a dramatic cost. Some of these costs are easy to calculate,
such as the fact that we spend roughly 10% of
our GDP on health care whereas America spends 15%.
Some of the costs are more difficult to put a value on,
such as Canadians' immunity from financial devastation
if they become ill and the stark reality that 40 million
Americans are uninsured or under-insured. We spoke of
the costs of administering our health care system, which
are a fraction of the costs in the U.S. For example, most
Canadian surgeons have one secretary who does all of the
surgeon's billing as a small part of the job. In contrast,
it is not uncommon for an American surgeon to employ
three or more individuals whose sole job is to negotiate
payments with insurance companies and administer a
complex billing process. We were asked what our average
receipts were for every dollar billed. When we answered
roughly 99 cents on the dollar, our American colleagues
were flabbergasted. The American system is so unwieldy
that Blue Cross of Massachusetts employs more people
to administer coverage for 2.5 million New Englanders
than are employed in all of Canada to administer single
payer coverage for 27 million Canadians.
But does the American health care dollar buy better
health? The answer is essentially no. Gord Guyatt, in a
systematic review of studies comparing health outcomes
in Canada and the United States, examined 10 recent
"high quality" studies. He reported that of the ten, five favoured outcomes in the Canadian system, two
favoured outcomes in the American system and three were equivocal (4).
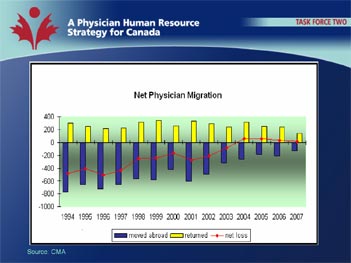
The myth that Canadian doctors are escaping to the U.S.
in droves still persists. I believe we dispelled that myth.
Data from the Canadian Institute of Health Informatics
show that the "brain drain" reversed in 2004. In 2001,
555 physicians left Canada whereas 334 returned. In
2004, 262 left and 317 returned and in 2005 185 left
and 247 returned.
|
We also addressed the issues of governmental involvement
in patient care. We emphasized that in our system
patients choose their own doctor and the government
does not participate in day-to-day care, nor do they collect
any individual patient information. We took pains
to indicate that everyone in our system receives the same
level of care. Finally we stressed that when polled 86 %
of Canadians supported or strongly supported public
solutions to make our public health care stronger.
|
A fair bit of the discussion was philosophical. We questioned
what the barometers were of a civilized society
and opined that one measure is the ability of a nation
to look after its sick. We questioned the right of insurance
companies to make large profits on the unfortunate
victims of illness. We underscored that Canada's health
care system, which fully looks after 32 million people,
costs roughly what the private-sector health insurance
companies make in profits in the United States. And we
talked of the medical mal-practice culture in the U.S.
compared to Canada. In the U.S. it is estimated that
court costs and judgments add 2 to 3% of GDP to the total medical tab (5).
|
Our American colleagues were stunned when we reported
the incomes of Canadian surgeons in the academic
sector. Without question, our surgeons are making a
much better living than they would as academic clinicians
in just about any American jurisdiction. With a
gross income of $335,000 (2006 CMA data), approximately
$100,000 in salary support for a new academic
recruit, a minimum of 20% protected time, average oncall
duties of one in six, virtually no time spent on sourcing
work, and malpractice premiums of $12,000 -- by all
measures, Canadian surgeons are doing well.
Finally, we discussed training and the looming HHR crisis
in both our countries. While both nations are under
the same strain with respect to physician shortages, we
are much better positioned to respond to this problem.
The root of the difference is the Balanced Budget
Amendment in the U.S. which has ostensibly thwarted
growth of residency programs. In contrast, Canada-wide,
the numbers of surgical residency positions has grown
from 1350 in 05-06 to 1550 in 08-09; an increase of
15%.
After one and one half hours of talks and a robust and
animated question period, the session closed. All five
of us, McLeod, Finley, Fitzgerald, Scully and Reznick
remained for a long time to accommodate individuals
who had additional questions for us. We were overwhelmed
by their interest, upset by the depth of concern
many expressed about their own system and immeasurably
proud to be Canadian.
Richard K. Reznick
R. S. McLaughlin Professor and Chair
(1)
http://thecaucus.blogs.nytimes.com/2009/08/18/death-panels- arent-the-half-of-it-says-senator-kyl/: accessed Nov. 9, 2009
(2) http://www.google.com/hostednews/canadianpress/article/ALeqM 5jRNEXbCDOJNCa_L56GCMqRDYehmw :
accessed Nov. 9, 2009
(3) www.hc-sc.gc.ca/hcs-sss/hhr-rhs/strateg/romanow-eng.php:
(accessed Nov. 8, 2009)
(4) Guyatt GH, Devereaux PJ, Lexchin J et al. A systematic
review of studies comparing health outcomes in Canada
and the United States. Open Medicine, Vol 1, No 1
(2007)
(5) http://network.nationalpost.com/np/blogs/francis/ archive/2009/05/12/health-care-lies-about-canada.aspx :
(accessed Nov. 9, 2009)
|